
Boost Your Energy In 5 Simple Steps
Do you know the difference between Golfer’s Elbow and Tennis Elbow?
Have you been suffering from elbow pain and wanted to know how to treat Golfer’s Elbow? Read on…
What Is Golfer’s Elbow?
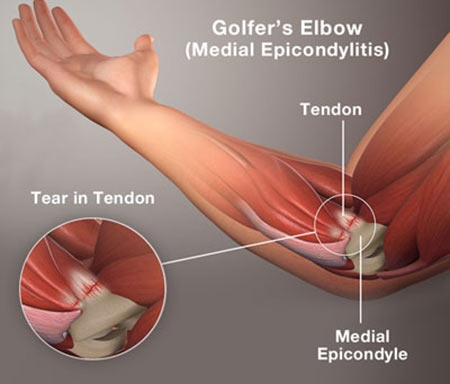
Golfer’s elbow is a condition quite similar to tennis elbow except it affects the muscle and tendon on the inside of the elbow.
This attachment is on the medial epicondyle and as such the medical term given is Medial Epicondylitis (ME) or flexor tendinopathy.
Golfer’s elbow is not a condition exclusive to golfers and is close to 6 times less common than tennis elbow.
Studies show that it is most common in middle age population and affects women more than men (Donaldson, et.al).
What Causes Golfer’s Elbow?
Golfer’s Elbow or ME, happens because of an inflammation of the tendon which attaches to the medial epicondyle (a bony structure of the humerus).
Flexor tendinopathy on the other side may have similar symptoms including pain and weakness but has no inflammation.
Both conditions can develop due to
- overuse (repetitive strain)
- or overloading of the muscles that are responsible for flexion of the wrist.
This is often due to faulty technique and biomechanics in
- throwing activities
- incorrect lifting techniques or
- occupational tasks that involve gripping and lifting.
This type of injury can occur because as there is not enough time for the muscle to rest between training or when work volumes are higher.
What Muscles Are Involved?
There are two muscles in the forearm – pronator teres and flexor carpi radialis – which are responsible for wrist flexion and pronation (turning the palm down). Both these muscles attach via tendons at the medial epicondyle, at the inside of the elbow.
When the wrist flexes (bends forward) under load the force at the attachment may be in excess of the tendon capability and as a result micro-tears occur.
In addition, when you are throwing a ball or object, this can also affect the same muscles, which is why repetitive actions such as this can bring on the symptoms of pain.
What Are The Symptoms of Golfer’s Elbow?
The main symptom is pain inside of the elbow (at the medial epicondyle near or at the location of the pronator teres attachment). The pain is made worse when you try to turn your hand inwards and down if you are holding your palm up against pressure.
If the continued activity makes it worse, the pain may spread down the front of the forearm to the wrist. You may also experience less grip strength compared to when uninjured.
It is not uncommon for this to progress and become a chronic condition. This can occur due to incomplete healing of the initial injury, poor blood flow or inadequate treatment.
How Is Golfer’s Elbow Diagnosed?
The diagnosis of Golfer’s Elbow is achieved by taking a thorough client history and examination of the area often using a number of special physical tests. These tests should be performed by a qualified health professional and include;
- Resisted wrist flexion and pronation; both tests will put increased force through the tendon, so if they reproduce the pain it is considered a positive test.
- Palpation of the muscle and tendon over the lateral epicondyle to identify tender areas.
It is important to also rule out if the Ulnar nerve or ligaments surrounding the elbow are involved. Usually, there is no need for an X-ray or MRI to diagnose this.
How Do I Treat Golfer’s Elbow?
Many of the treatments for medial epicondylitis are based on the management protocol for tennis elbow. Few studies have been conducted specifically on medial epicondylitis.
In the acute stage the preferred management/treatment would include rest from the aggravation activity, ice, compression and a visit to the GP or physiotherapist for diagnosis and more specific treatment.
- Rest from the aggravating activity is very important early on. This can really impact how successful treatment will be and it has also shown to be very important in preventing the condition to become chronic
- Ice can be applied to the area post activity to ‘settle’ inflammation and manage pain.
Nonsteroidal anti-inflammatory drugs (NSAIDs) may be suggested by the physician to manage the inflammation in the acute stage.
For patients who present with a more chronic flexor tendinopathy the initial treatments are nonsurgical and include:
- Physical therapy
- Shockwave therapy
- Braces and
- Steroid injections.
A good physiotherapist or remedial massage therapist can apply effective soft tissue techniques that help decrease the tension in the muscle tendon unit as well as some specific cross fibres techniques to work on the affected part of the tendon.
They can also address areas that may be contributing to the problem such as the neck or shoulder and go over in detail what some of the aggravating factors including ergonomics and training load.
In addition to seeing a professional there are exercises that you can do to treat yourself at home. Your therapist is the best person to talk to about this to personalise your treatment.
With proper treatment and rest, most clients will heal within 12 months.
What Can I Do Now?
If you would like to see one of our therapists for how to treat Golfer’s Elbow, you can call us on 02 8021 8430 to make an appointment or book here.
References:
- Brukner, P., and Khan, K. (2006) Clinical Sports Medicine.3rd Ed. Sydney: McGraw-Hill Book Company
- Donaldson, O., Vannet, N., Gosens, T. and Kulkarni, R. (2014) ‘Tendinopathies Around the Elbow Part 2: Medial Elbow, Distal Biceps and Triceps Tendinopathies’, Shoulder & Elbow, 6(1): 47–56. doi: 10.1111/sae.12022
- Mayo Clinic (no date) Golfer Elbow. Available at:
https://www.mayoclinic.org/diseases-conditions/golfers-elbow/symptoms-causes/syc-20372868 (Accessed: 15 February 2020)
Related posts





